
You looked up your BMI, and the number isn't where you want it to be. Maybe it's nudging into the overweight range, maybe it's firmly in the obese category, or maybe your doctor brought it up during a check-up. Whatever the context, you're looking for real answers — not vague advice to "eat less and move more."
This guide goes deeper than most. We'll cover what actually moves your BMI, what the science says about male vs female BMI differences, why the standard calculator fails weightlifters, what you need to know if you're considering Wegovy, and a practical week-by-week framework to start lowering your BMI today.
What BMI Actually Measures (and What It Misses)
Body Mass Index is calculated by dividing your weight in kilograms by your height in metres squared. That's it. No muscle measurement, no bone density, no fat distribution — just the ratio of mass to height. It was developed by Belgian mathematician Adolphe Quetelet in the 1830s as a tool for measuring population averages, not individual health.
Despite its limitations, BMI remains the most widely used screening tool in clinical medicine. It's fast, free, and requires no equipment. It also correlates reasonably well with metabolic risk at the population level, which is why public health researchers and clinicians still use it.
Where it breaks down:
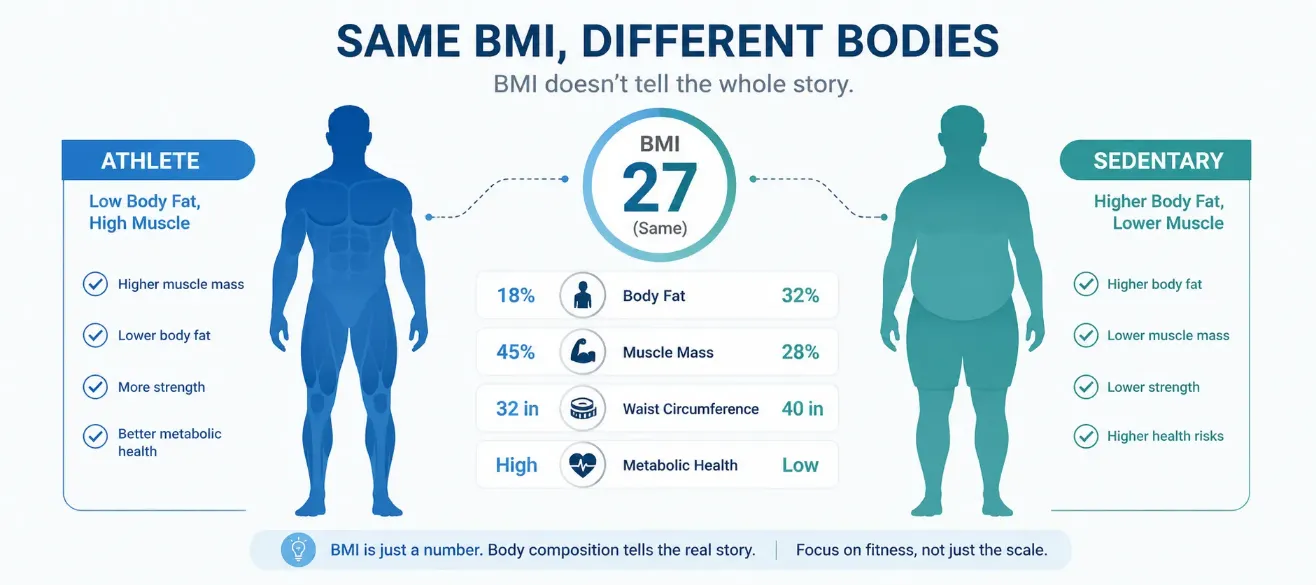
- Athletes and weightlifters — muscle is denser than fat, so someone with 10% body fat and significant muscle mass can register as "overweight" or even "obese" on the BMI scale
- Older adults — muscle loss (sarcopenia) means an elderly person can have a healthy BMI while carrying excess fat
- Different ethnic groups — some Asian populations carry metabolic risk at lower BMI thresholds than the standard WHO cut-offs suggest
- Men vs women — women naturally carry 6–11% more body fat than men at the same BMI due to hormonal and reproductive biology
Knowing these limitations doesn't mean dismissing BMI — it means using it as one signal in a broader picture. For most people who aren't professional athletes, a BMI above 25 does correlate with elevated health risks, and reducing it is a legitimate health goal.
Male vs Female BMI: Why the Same Number Means Different Things
One of the most significant gaps in most online BMI content is a proper discussion of how male and female BMI differ — not just in calculation (the formula is identical), but in what the result actually means for health.
Why Women Naturally Carry More Fat
Biological sex influences fat storage in fundamental ways. Estrogen promotes fat deposition — particularly in the hips, thighs, and breasts — as a biological reserve for reproductive function. This is not a flaw; it's physiology. Women typically have 20–25% body fat in the healthy range, while healthy men typically fall between 10–20%.
This means a woman with a BMI of 23 may have meaningfully more body fat than a man with a BMI of 23, yet both sit within the "healthy" category. The health implications are different, too — female fat storage patterns (subcutaneous, around the hips and thighs) are associated with lower cardiovascular risk compared to the abdominal (visceral) fat that men tend to accumulate.
How to Lower BMI as a Woman
Women face specific hormonal dynamics that affect weight management:
- Menstrual cycle fluctuations — water retention during the luteal phase can cause 1–3 kg fluctuations that affect BMI readings. Weigh yourself at the same phase each month for accurate tracking.
- Perimenopause and menopause — declining estrogen shifts fat distribution toward the abdomen, increasing health risk even without a change in BMI. Strength training becomes especially important during this period.
- Calorie needs — women generally have lower BMR (Basal Metabolic Rate) than men due to less muscle mass, meaning calorie deficits need to be more carefully managed to avoid nutritional deficiencies.
How to Lower BMI as a Man
Men tend to lose weight faster initially due to higher muscle mass and testosterone, but face their own challenges:
- Visceral fat accumulation — abdominal fat is more metabolically active and responds well to calorie restriction and cardiovascular exercise, often producing faster visible results than subcutaneous fat
- Waist circumference — for men, a waist over 102 cm (40 inches) is a stronger predictor of metabolic disease than BMI alone
- Alcohol — men statistically consume more alcohol than women, and alcohol is a hidden source of significant calories that directly increases visceral fat
BMI for Weightlifters and Athletes: Why Your Number Lies
If you lift weights seriously, play a contact sport, or have built significant muscle over years of training, your BMI is almost certainly inaccurate as a health metric. This is not a minor footnote — it's a fundamental flaw of the measure for this population.
Consider a 180 cm man who weighs 95 kg with 12% body fat. His BMI calculates to 29.3 — technically "overweight." But his fat mass is only about 11.4 kg. By any reasonable measure of health, he is fit. The BMI formula cannot distinguish his 83.6 kg of lean mass from stored fat.
Better Metrics for Muscular Individuals
| Metric | Method | Accuracy | Best For |
|---|---|---|---|
| DEXA Scan | Imaging | Very high (~1-2%) | Athletes, clinical use |
| Skinfold Calipers | Manual measurement | Medium (~3-5%) | Gym tracking, coaches |
| Navy Tape Method | Neck + waist circumference | Medium (~3-4%) | Military, practical use |
| Waist-to-Height Ratio | Tape measure | Good for cardiometabolic risk | General health screening |
| BMI | Weight ÷ height² | Low for athletes | Population screening only |
What the Marine Corps Uses Instead of BMI
The US Marine Corps illustrates this problem well. While general military fitness standards reference BMI as a rough screening gate, the Marine Corps body composition program actually uses a tape-measure method — specifically the Wright Method — that calculates body fat percentage from neck and abdominal circumference. Male Marines must maintain under 18% body fat; female Marines under 26%. A highly muscular Marine who exceeds weight-for-height limits can still pass the body composition assessment with acceptable body fat percentage.
This is an important real-world example: even institutions that rely on mass screening have moved past pure BMI when individual assessment is needed.
BMI and Wegovy: What You Need to Know
Interest in Wegovy (semaglutide 2.4 mg) has grown significantly since its approval for chronic weight management. If you're researching whether Wegovy is an option for you, BMI is the primary clinical gating criterion — and understanding it matters.
Wegovy BMI Requirements
In most markets, including the UK, US, and New Zealand, healthcare providers can prescribe Wegovy when:
- Your BMI is 30 or higher (obese range), regardless of other conditions, or
- Your BMI is 27 or higher (overweight) with at least one weight-related comorbidity — such as type 2 diabetes, high blood pressure, high cholesterol, obstructive sleep apnoea, or cardiovascular disease
These thresholds mean that if your BMI is 28 with no other conditions, you may not qualify, but if your BMI is 28 and you have elevated blood pressure, you likely would. A healthcare provider will assess your full clinical picture — BMI is a necessary but not sufficient criterion.
Wegovy Is a Tool, Not a Replacement for Lifestyle
Clinical trials for semaglutide show an average weight loss of 15–17% of body weight over 68 weeks — a genuinely significant result. However, trials also showed that much of the weight returned within 12 months of stopping the medication when lifestyle changes weren't maintained. Wegovy works best as part of a comprehensive approach that includes the nutritional and exercise strategies outlined later in this article.
The Science-Backed Steps to Actually Lower Your BMI
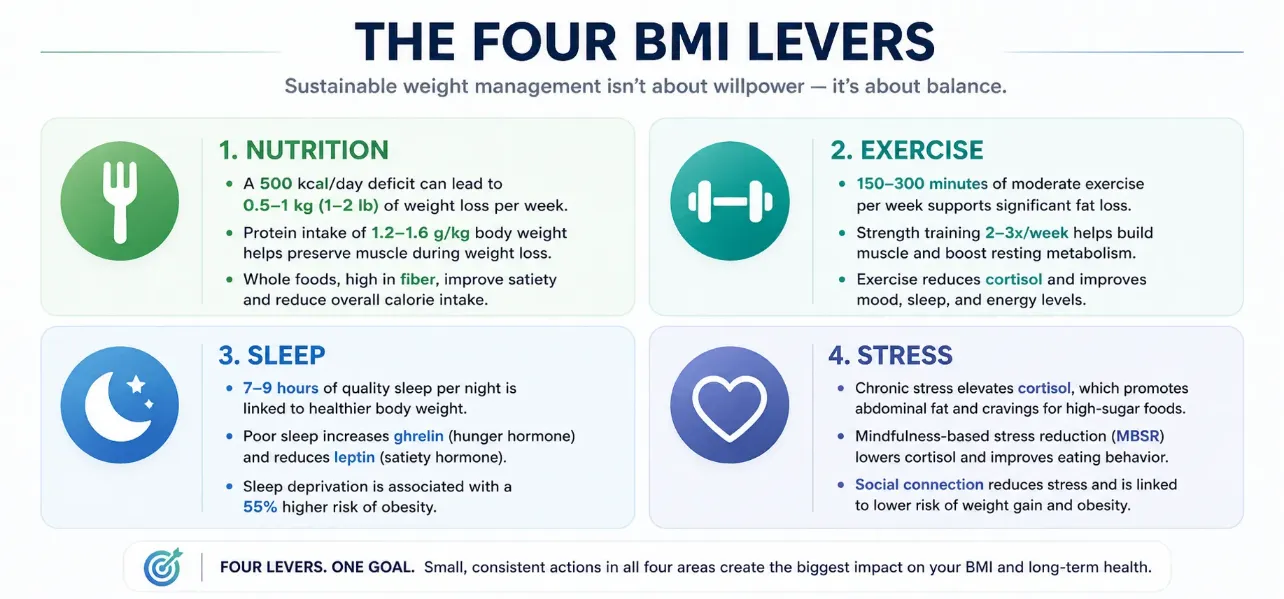
Lowering BMI requires reducing body fat — specifically, creating the conditions for your body to use stored fat as energy. There are four main levers: nutrition, movement, sleep, and stress management. Each one individually produces modest effects. Combined, they create sustainable, compounding change.
1. Create a Moderate Calorie Deficit (Not a Crash)
Fat loss requires energy deficit — consuming fewer calories than you burn. However, the size of that deficit matters enormously. Very large deficits (more than 1,000 kcal/day) cause rapid muscle loss alongside fat loss, lower your resting metabolic rate, and are rarely sustainable beyond a few weeks.
The evidence-backed sweet spot for most people:
- A deficit of 300–500 kcal per day produces 0.3–0.5 kg of fat loss per week — enough to meaningfully move BMI without sacrificing muscle or triggering metabolic adaptation
- Prioritise protein (1.6–2.2g per kg of body weight) to preserve muscle mass during the deficit
- Don't eliminate food groups — restriction-based thinking leads to binge-restrict cycles that derail progress. Focus on satiety-dense whole foods instead.
2. Combine Resistance Training with Cardio
This is the single most important exercise insight most people miss. Cardio alone burns calories during the session, but resistance training builds muscle tissue that increases your resting metabolic rate over time — meaning you burn more calories even at rest.
- Resistance training 2–4× per week — full-body compound movements (squats, deadlifts, rows, presses) are most efficient for preserving muscle during weight loss
- Moderate-intensity cardio 150+ minutes per week (walking, cycling, swimming) — consistent cardiovascular activity is associated with lower visceral fat independent of weight change
- NEAT (Non-Exercise Activity Thermogenesis) — increasing daily movement through walking, taking stairs, and standing is often more impactful than structured cardio alone for sedentary individuals
3. Fix Your Sleep First
This is the step most "how to lower BMI" articles completely skip, and it's one of the most impactful changes you can make. Sleep deprivation directly disrupts the hormones that regulate appetite and fat storage:
- Ghrelin (hunger hormone) rises significantly after just two nights of poor sleep — increasing appetite by roughly 24% in some studies
- Leptin (satiety hormone) is suppressed, meaning you feel less full even after eating
- Cortisol rises with chronic sleep deprivation, promoting visceral fat storage around the abdomen
- People sleeping under 6 hours per night have consistently higher BMI in population studies — and the relationship is dose-dependent: less sleep, higher BMI
Targeting 7–9 hours of consistent sleep is not optional if you're trying to manage weight. It's arguably more impactful than any specific diet strategy for many people.
4. Manage Stress Systematically
Chronic psychological stress elevates cortisol, which promotes fat deposition — specifically in the abdomen — and drives cravings for calorie-dense, high-sugar foods. Stress eating is not a willpower failure; it's a neurobiological response to cortisol and reward-seeking pathways.
Evidence-backed stress reduction strategies that directly support BMI reduction:
- Mindfulness-based stress reduction (MBSR) — 8-week programs have shown measurable reductions in cortisol and improved eating behaviour in controlled trials
- Regular physical activity — works double duty as both a calorie burner and a powerful cortisol regulator
- Social connection — loneliness and isolation are independent risk factors for weight gain and obesity
5. Address Hidden Calorie Sources
Many people eat reasonably at mealtimes but consistently underestimate the calories from beverages, condiments, and snacking. These "invisible calories" are frequently responsible for why a person feels like they're eating well but not losing weight:
- Alcohol — 7 kcal per gram (more than carbohydrates or protein). Two glasses of wine add roughly 300-400 kcal with no nutritional value
- Liquid calories — sugary coffees, smoothies, and juices can add 200-600 kcal per day without triggering significant satiety
- Ultra-processed foods — highly palatable, engineered to be over-consumed, and calorie-dense relative to their satiety value
- Condiments and cooking fats — a tablespoon of olive oil adds 120 kcal. This adds up quickly when cooking several meals daily
6. Track Progress the Right Way
BMI changes slowly — most people won't see a meaningful shift in less than 4-6 weeks of consistent effort. Day-to-day weight fluctuates by 1-3 kg due to water, food volume, and hormonal factors. Obsessing over daily weigh-ins is counterproductive.
Better tracking approach:
- Weigh yourself at the same time each week (morning, after using the bathroom, before eating) and track a weekly average
- Take monthly waist measurements alongside BMI — waist circumference is often a more sensitive indicator of progress than weight alone
- Use photos at regular intervals — visible body composition changes often outpace what the scale shows
- Track non-scale victories: energy levels, sleep quality, strength in the gym, resting heart rate
Realistic Timeline: How Fast Will Your BMI Drop?
One of the most frustrating things about mainstream weight loss advice is that it either promises unrealistic speed or provides no timeline at all. Here is what the science actually supports:
| Timeframe | Expected Change | What's Actually Happening |
|---|---|---|
| Week 1–2 | 0.5–2 kg weight loss | Mostly water and glycogen depletion — not fat. Don't be discouraged if initial losses slow. |
| Week 3–6 | 0.3–0.7 kg/week true fat loss | Consistent calorie deficit taking effect. BMI begins to move by 0.1–0.3 points per week. |
| Month 2–3 | 1–2 BMI points reduction | Visible body composition changes. Waist measurement often improves faster than BMI suggests. |
| Month 4–6 | 2–4 BMI points reduction | Metabolic adaptation may slow progress — consider a 1–2 week diet break to reset leptin levels. |
| 6–12 months | 4–8+ BMI points (with consistency) | Long-term lifestyle changes embedding. Risk of regain is highest here — focus on habit durability. |
If your BMI is currently 32 and your goal is 24, you're looking at 8 BMI points of change. At a consistent rate of 1-2 points every 2-3 months, that's a 12-18 month journey. That is not discouraging — it means the changes that get you there are sustainable lifestyle shifts, not crash interventions that fail within weeks.
Frequently Asked Questions
The Bottom Line
Lowering your BMI is not about extremes. It's not about eliminating carbs, doing two-a-day workouts, or counting every calorie for months on end. It's about consistently creating the conditions — a moderate energy deficit, regular movement, adequate sleep, managed stress — that allow your body to reduce stored fat over time.
The people who succeed long-term are not the ones who try hardest for six weeks. They're the ones who find the minimum effective dose of change they can sustain for twelve months. Start with one lever, get that working, then add the next.
And if you're unsure where you stand, start with the number itself — use the CalcMeter BMI Calculator to see your current BMI and category, then work backwards from there.